Anesthesia for a Mediastinal Mass (Preview)
Presented by Dr. Keith Herring and Dr. Davide Cattano, University of Texas Health Science Center at Houston.
|
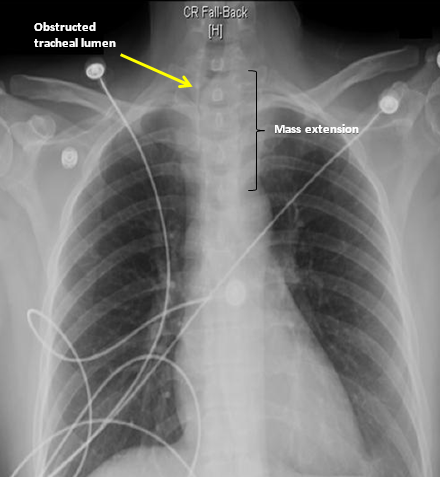
Case presentation: A couple of months ago we presented a highly challenging case of a patient who was scheduled to undergo an urgent biopsy and possible resection of advanced mediastinal mass. The patient was a 38 y.o. female who came to the emergency room (ER) with a two month history of progressively worsening cough, dysphonia and dysphagia. One week prior to admission her symptoms worsened, and she had developed hemoptysis. Chest radiograph (CXR) and contrast-enhanced computed tomography (CT) revealed a 4.5 x 4 x 4.3 cm homogenous mass displacing the left inferior pole of the thyroid gland, and a compression of the extrathoracic trachea with a slit-like appearance (Figures 1 and 2). The erosion of the mass into the trachea could not be excluded. There was a significant mass effect on the esophagus, with the collapse of the lower cervical and upper thoracic segments. The ER immediately transferred the patient to the intensive care unit (ICU).
Figure 2.
The patient’s past medical history was unremarkable, with the exception of the family history of non-Hodgkin’s lymphoma. Physical examination revealed a firm mass of the left lower neck, extending to the left thyroid lobe, and obscuring the neck anatomical landmarks. The patient had mild, predominantly inspiratory, stridor, with notable subcostal and suprasternal retractions. Vital signs were stable: non-invasive blood pressure (NIBP) 122/63 mm Hg, heart rate (HR) 85/min, and SpO2 100% on 2 l/min nasal cannula; BMI was 29.3 kg/m2. The airway exam was unremarkable, with the Mallampati score of I. The EKG showed normal sinus rhythm, and the transthoracic echocardiogram (TTE) revealed normal valvular function with the EF of 50-55%.
The following questions were offered for discussion:
|
|
|



Join SHANA or Log in to view more/discuss on Forum.

FEATURED
QUICK CONNECT
SUGGEST and SUBMIT
