What’s going on in there?
By Laura Cavallone, MD, MSCI
Associate Professor and Vice Chair for Research of the Department of Anesthesiology at the University of Mississippi Medical Center, Jackson, Mississippi, USA

Figure 1
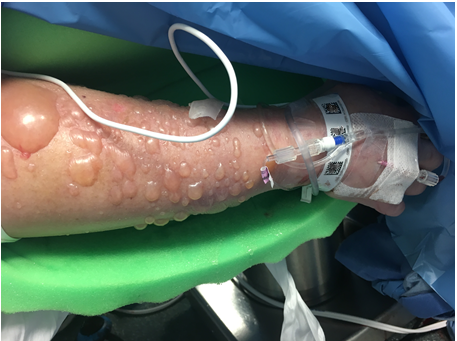
Figure 2
Questions
- What do these two pictures have in common and what do they have to do with Head and Neck surgery?
Answer: ... Answers available for SHANA members
- What do you think is the cause of the injuries in Figure 1?
Answer: ... Answers available for SHANA members
- How do these types of injury (Figure 1) occur?
Answer: ... Answers available for SHANA members
- What do you think is the cause of the injury in Figure 2?
Answer: ... Answers available for SHANA members
Take home message
In long, involved cases, when areas of the body are covered by drapes and/or wrapped in protective foam and cannot be regularly inspected (as is often the case in head and neck surgeries with the bed turned 180 degrees), the risk exists of serious injuries occurring with different mechanisms. Such injuries may go unnoticed until the end of the case, with critical consequences adding to the risks strictly related to the surgeries that these patients are undergoing. Positioning of the patient with head “away from the anesthesia location” and with arms tucked along the body, frequently occurs in major head and neck surgery, and the associated risks need to be recognized. Other potential injuries in this category include injuries due to mechanical compression (including nerve injuries) and ischemic injuries to the hand (or more specifically to the fingers receiving vascular supply from radial artery) when an arterial line (A-line) is in place. To prevent some of these injuries it may be advisable to consider foot lines (foot IV lines and dorsalis pedis A-line) in order to improve the possibility to monitor line sites intraopertively form the anesthesia location. To prevent finger ischemia in the territory supplied by the radial artery, when radial A-line is in place, consideration should be given to positioning a pulse-oxymetry probe on the index finger on the side of the radial A-line.
References
- Samuel M Sanders, Stephanie Krowka, Andrew Giacobbe, Leslie J Bisson.
Third-degree burn from a grounding pad during arthroscopy. Arthroscopy. 2009 Oct;25(10):1193-7. doi: 10.1016/j.arthro.2008.11.003
- Saaiq M, Zaib S, Ahmad S.
Electrocautery burns: experience with three cases and review of literature. Ann Burns Fire Disasters. 2012 Dec 31;25(4):203-6
- Hahn-Sol Bae, Mu-Young Lee, Ji-Ung Park.
Intraoperative burn from a grounding pad of electrosurgical device during breast surgery: A CARE-compliant case report. Medicine (Baltimore). 2018 Jan;97(1):e8370. doi: 10.1097/MD.0000000000008370.
- Jason Chui, John M Murkin, Karen L Posner, Karen B Domino.
Perioperative Peripheral Nerve Injury After General Anesthesia: A Qualitative Systematic Review. Anesth Analg. 2018 Jul;127(1):134-143. doi: 10.1213/ANE.0000000000003420
- Valentine RJ, Modrall JG, Clagett GP.
Hand ischemia after radial artery cannulation. J Am Coll Surg. 2005 Jul;201(1):18-22. doi: 10.1016/j.jamcollsurg.2005.01.011
- Kim D, Arbra CA, Simon Ivey J, Burchett P, Gonzalez G, Herrera FA.
Iatrogenic Radial Artery Injuries: Variable Injury Patterns, Treatment Times, and Outcomes. Hand (N Y). 2019 May 1:1558944719844348. doi: 10.1177/1558944719844348.

FEATURED
QUICK CONNECT
SUGGEST and SUBMIT
